


Adolescent Health Care
WHEC Practice Bulletin and Clinical Management Guidelines for Healthcare Providers. Educational grant provided by Women's Health and Education Center (WHEC)
Adolescent is a time of psychosocial, cognitive, and physical development as young people make the transition from childhood to adulthood. The Women's Health and Education Center believes healthcare professionals have an obligation to provide the best possible care to respond to the needs of their adolescent patients. This care should at a minimum, include primary and preventive care and comprehensive reproductive health services such as sexuality education, counseling, mental health assessment, diagnosis and treatment regarding pubertal development, access to contraceptives and abortion, pregnancy-related care, prenatal and delivery care, and diagnosis and treatment of sexually transmitted diseases. Adolescent girls, in particular, are confronted with numerous challenges, and the decisions they make can have both short- and long-term consequences for their health and well-being. Guidance from a physician can greatly facilitate a young girl's healthy transition to adulthood. Healthcare professionals can provide preventive guidance to both parents and adolescents.
The purpose of this document is to assist healthcare providers in understanding an adolescent's unique developmental stage that dictates the framing of preventive services. The delivery of preventive services to adolescents differs from the delivery of preventive services to adults. Furthermore, not all adolescents of the same age are at the same stage of development, thus necessitating further examination of adolescent's physical, sexual, psychosocial, and cognitive development. Understanding the milestones and developmental stages of adolescence is beneficial to obstetricians and gynecologists treating adolescents. Comprehensive services may be delivered to adolescents in a variety of sites, including schools, physician offices, and community-based and other health care facilities. Legal barriers that restrict the freedom of healthcare practitioners to provide these services are also discussed.
Female Adolescent Development:
Sexual Development: Thelarche, or breast budding, the first sign of secondary sexual development in most adolescent females, occurs for most young girls in North America at age 8-10 years. Production of low amounts of estrogen stimulates long bone growth, with a peak height growth of 9 cm per year. When high levels of estrogen are produced, breast development progresses, long bone growth decelerates, and the epiphyses close. Menarche occurs during this deceleration phase. On average, the first menses 12-13 years, with regular ovulation established by approximately 20 cycles later. The average duration of puberty is 4 years, with a range of 1.5 years to 8 years. Data from a large-scale cross-sectional study indicate that at every age and for the development of each pubertal characteristic, African-American girls are more advanced than White girls. Pubic hair or breast development requires evaluation only when it occurs before age 7 years in non-African-American girls and before age 6 years in African-American girls. If there is any uncertainty, an evaluation should be performed and referrals made as appropriate. In addition, tempo and sequence aberrancies during an otherwise established pubertal process should be included for evaluation of delayed or precocious sexual development.
Psychosocial and Cognitive Development: Adolescent is a prolonged period of transition during which a young person's expanding horizons, self-discovery, and quest for independence lead to the formation of a separate and distinct identity. It is particularly challenging because the processes of physical, psychologic, and cognitive development occur on separate tracks, with different timetables, which rarely are synchronous. Cognitive development tasks allow her to 1) understand the consequences of present behaviors on future health outcomes and make crucial decisions about the future, 2) understand the saliency of risks and internalize those risks, and 3) form and maintain stable and healthy relationships while evolving and learning to communicate a value system of her own. The adolescent often believes that she is different from other and therefore, not liable to the risks that threaten her peers. As the girl progresses through adolescence, she becomes increasingly capable, both cognitive and emotionally, of comprehending abstract ideas, relating present actions to future outcomes, and understanding the consequences of her own behaviors. Thus, the clinical approach to counseling a younger adolescent will differ from the approach taken with an older adolescent or an adult.
Teen Pregnancy: Understanding the Social Impacts
Adolescent's Right to Refuse Long-term Contraceptives:
Various forms of reversible hormonal contraceptives are now widely available, and they are being widely promoted for use in women, including adolescents who will not or cannot use other contraceptive methods. The implantable and injectable progestins also are viewed by some individuals as a method of limiting adolescent pregnancies. This raises concerns about the adolescent's right to accept or refuse a method of contraception against parental request and about the potential coercive use of such contraceptives in minor. Because the involvement of a concerned adult can contribute to the health and success of an adolescent, policies in health care setting should encourage and facilitate communication between a minor and her parent(s), when appropriate. Parents who feel their adolescent daughter is at risk for an unintended pregnancy may request that the physician administer long-term contraceptives to their daughter against her wishes. Healthcare agencies, social workers, and guardians may make similar requests. The physician, however, should acknowledge that the adolescent is the patient and has the final decision and right of free choice. The role of the physician in providing care to an adolescent is more than that of a technician who administers a contraceptive method. In the situation in which an adolescent refuses long-term contraceptives, the physician should explore thoroughly the reasons for her refusal. This process may help correct misinformation and allay fears.
Physicians providing care should have knowledge of their state laws regarding minor's rights and also should be aware that adolescents have constitutional rights to privacy and to make reproductive decisions. The U.S. Supreme Court first ruled more than 35 years ago that the 14th Amendment protects the rights of minors as well as those of adults. The rights of minors are subject to more limitations than the rights of adults; however, a subsequent ruling held that minors have a constitutional right to privacy that includes the right to obtain contraceptives. There are no state laws that require parental involvement for a minor to obtain medical care in connection with contraceptive services. Information also should be provided on how to avoid sexually transmitted diseases, including human immunodeficiency virus (HIV) infection, with both short- and long-term contraceptive methods. The physician also should assess the reasons for the adult's request so that appropriate intervention can be instituted. If the physician determines or suspects that the disagreement between the minor and adult, especially parent or guardian, over a contraceptive choice reflects a deeper or more long-standing conflict, the physician may make a referral to an appropriate practitioner or agency. If the parent or guardian is requesting long-term contraception for an adolescent who is incapable of giving informed consent, the decision to use long-term contraception should be based on a careful assessment. This may involve a multidisciplinary team that includes an advocate appointed for the impaired adolescent.
Finally, regardless of whether an adolescent selects or refuses a long-term contraceptive method, the physician should remain available to address related health concerns. This includes a commitment to offer continuing contraceptive care, periodic evaluation for sexually transmitted diseases, screening via Pap test and HPV screening.
Cervical Cancer Screening in Adolescents:
The American Cancer Society (ACS) recently published a recommendation that cervical cancer screening should begin approximately 3 years after the onset of vaginal intercourse or no later than age 21 years. Once initiated, screening should occur annually for adolescents. This recommendation is based on the consensus of a national panel of experts who reviewed evidence and concluded that there is little risk of missing an important cervical lesion within 3-5 years after initial exposure to human papillomavirus (HPV). The ACS further supports this recommendation by stating that screening less than 3 years after the onset of vaginal intercourse may result in over-diagnosis of cervical lesions, which often regress spontaneously, and that inappropriate intervention may cause more than good. The ACS recommendation states that it is critical for adolescents who may not need cervical cytology testing to receive gynecologic health care, including preventive measures such as sexually transmitted disease (STD) testing in sexually active patients. Adolescent females have a higher prevalence of abnormal Pap test results (atypical squamous cells of undetermined significance or ASCUS and above) when compared with adult females. However, the severity of lesions tends to be lower in adolescents. High-grade squamous intraepithelial lesions (HSIL) still do occur in adolescents. Behavior that may place adolescent patient at greater risk for HPV infection, obtaining a complete and accurate sexual history is, therefore, critical.
Human Papillomavirus (HPV) Vaccine: it is estimated that targeted HPV protection with the bivalent or quadrivalent vaccine would prevent most high-grade pre-cancerous lesions (CIN II or CIN III) and invasive cancers. The quadrivalent vaccine would also prevent most genital warts. HPV infection evades the immune system through a variety of mechanisms. HPV infection leads to down regulation of interferon expression and regulatory pathways, which subsequently prohibits the activation of cytotoxic T-lymphocytes. Approximately 75%-90% of HPV infections will clear within a year of initial infection. Clearance is mediated mostly by the natural desquamation of epithelial cells, and in part, by low-levels of neutralizing antibody responses to the specific HPV L1 epitope. Specific HPV types are associated with squamous intraepithelial lesions. HPV 16, 18, 45, and 31 cause over half of the low grade lesions, and about 65% of the high grade lesions. HPV 6 and 11 cause 12% of low grade lesions and approximately 80% of genital warts. Up to 40% of patients are infected with more than one HPV type. HPV 16 and 18 are associated with approximately 50% and 20% of cervical cancers, respectively. HPV 45 and 31 are the next most common HPV types associated with cervical cancer, accounting for another 5% each. The first peak of oncogenic HPV infection occurs between the ages of 15 to 25 years, with a secondary peak in the sixth decade of life. Since virus-like particles (VLPs) are recombinant proteins, manufactured in benign biologic systems (yeast and Baculovirus), they have no known oncogenic or disease-causing potential. The currently suggested immunization schedule is in girls and women 9 to 26 years of age. Quadrivalent HPV 6/11/16/18 L1 VLP vaccine (Gardasil) is administered in three doses at 0, 2, 6 months. The duration of immunity is unknown. The potential strategy of using HPV vaccine in men to prevent cervical cancer in women is being planned, although vaccine efficacy in males is unknown. Studies of male vaccination to prevent HPV-associated cancers occurring in men are underway.
High risk adolescents often have difficulty obtaining affordable healthcare. They are, therefore, more likely to receive episodic care and have difficulty in returning for routine follow up care. In the adolescent, noncompliance with follow up appointments for abnormal Pap test results ranges from 25% to 66%. The Pap test is a screening tool, not a diagnostic tool. Those patients with abnormal cytology should be counseled and monitored closely. It is important to avoid aggressive management of benign lesions because most cervical intraepithelial neoplasia lesions of CIN I and CIN II regress. An acceptable option is follow-up without initial colposcopy using a protocol of repeat cytologic testing at 6- and 12-month intervals with a threshold, or of HPV DNA testing at 12 months with a referral for colposcopy if test results are positive for high-risk HPV DNA. Cervical intraepithelial neoplasia (CIN) II represents a significant abnormality that typically requires therapy. It can be managed in adolescents with either ablative or excisional therapy or observation.
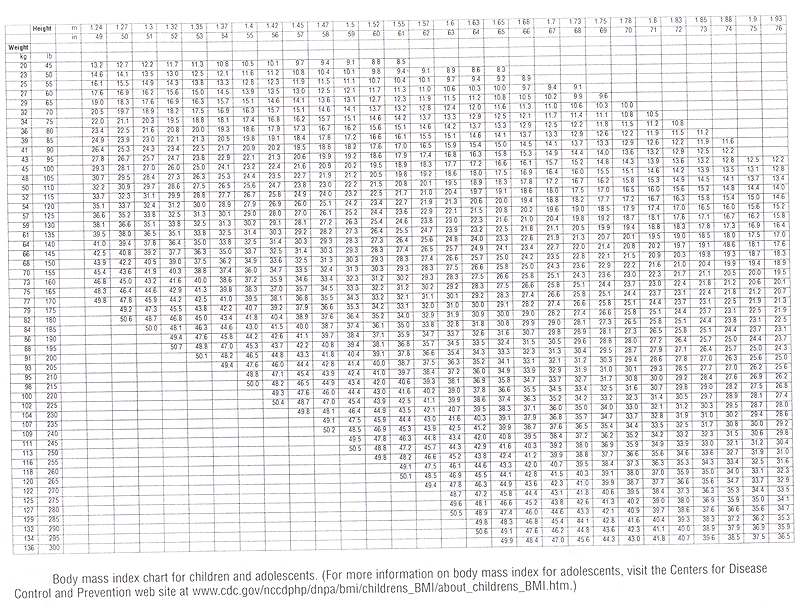
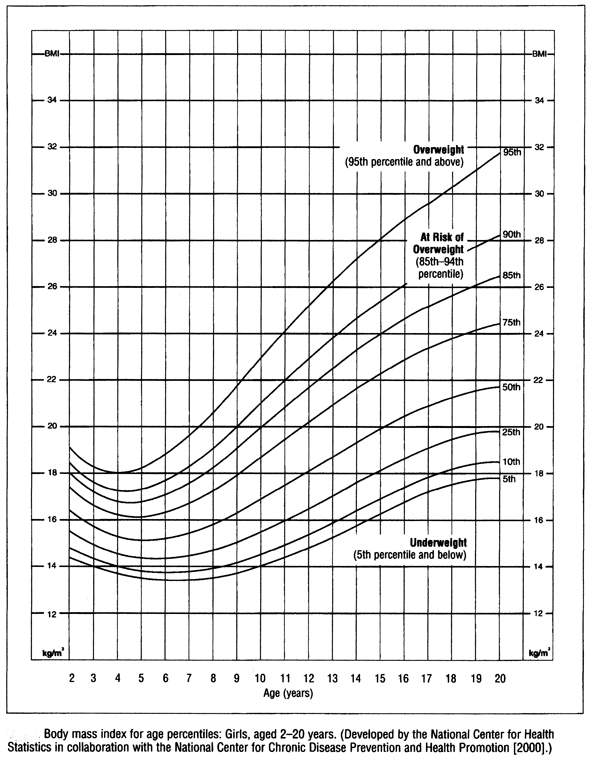
Overweight Adolescents:
The number of overweight adolescents has grown to epidemic proportions in the United States. Adolescent females who are overweight have significant health sequelae. Adolescents with a Body Mass Index (BMI) greater than or equal to the 95th percentile for age should have an in-depth dietary and health assessment to determine psychological morbidity and risk for future cardiovascular disease. The Centers for Disease Control and Prevention (CDC) defines an adolescent as overweight if she has a BMI greater than or equal to the 95th percentile for age -- Body Mass Index for Age Percentiles. For example, a girl aged 16 years whose height is 60 inches and weight is 155 pounds has a BMI of 30.3; therefore she is considered to be overweight. An adolescent whose BMI is equal to or greater than the 85th percentile for age, but less than the 95th percentile for age is considered by the CDC to be at risk for becoming overweight. According to National Health and Nutrition Examination Survey (NHANES) 2003-2004 data, 16% of females aged 12-19 years were considered overweight. By comparison, only 6% of females aged 12-19 years were considered overweight in the NHANES study conducted in 1971-1974. There are substantial racial differences in the prevalence of overweight for adolescents. Specifically, Latino, Mexican-American, Asian/Pacific Islander, and black populations are more likely to be overweight or at risk for overweight in adolescence than the white population.
{kind=link}
{kind=link}
Overweight adolescents often experience significant low self-esteem and depression. Among adults who are overweight during childhood, there is an increased relative risk of 1.5 of all-cause mortality and 2.0 of cardiovascular disease mortality. Hypertension, sleep apnea, dyslipidemia, increased fasting insulin levels, and sudden death have been associated with being overweight. More recently, overweight adolescents have been shown to be at increased risk of type 2 diabetes. Furthermore, a variety of orthopedic complications occur in overweight adolescents, such as slipped capital femoral epiphysis and Blount's disease (a growth disorder of the shin bone that causes the lower leg to angle inward). Overweight adolescents face increased morbidity and mortality later in their reproductive lives, such as: irregular menses -- amenorrhea, oligomenorrhea, or menometrorrhagia; polycystic ovary syndrome and pregnancy-related complications. For overweight adolescents at risk of pregnancy, it is important to balance the risks and benefits of combination oral contraceptives, including the risks from pregnancy. Consideration should be given to progestin-only oral contraceptives and intrauterine methods when counseling overweight adolescents regarding contraceptive choices. Women who weigh more than 90 kg may have a disproportionately higher likelihood of contraceptive failure with the transdermal contraceptive patch. No changes in efficacy have been shown with the vaginal ring regardless of patient weight. Although injectable contraception has not been demonstrated to decrease contraceptive efficacy based on weight, it has been associated with weight gain. Most adolescent pregnancies (80%) are unintended. Obesity is associated with increased risk of diabetes, hypertension, preeclampsia, stillbirth, neonatal death and increased risk of cesarean deliveries and the surgical complications.
Prevention: parents play a significant role, and healthcare providers should promote healthy eating and physical activity to adolescent patients and their parents during routine preventive health care visits. Often, collaboration with a mental health professional is indicated. Increased activity, decreased television viewing and computer games have been shown to reduce and adolescent's weight. There are limited data to document the efficacy of prescription medications or over-the-counter drugs for weight loss in adolescents. The role of surgical intervention for overweight adolescents has yet to be established, but some recent studies have suggested that surgical weight loss improves the early mortality experienced by these adolescents. Bariatric surgery currently is recommended for adolescents who have a BMI greater than 40 and have comorbid conditions. Those who may be candidates for bariatric surgery should be referred to a multidisciplinary weight management team with expertise in treating overweight adolescents.
Mental Health Promotion in School
Adolescent Suicide Risk Assessment and Prevention:
Suicide is the third leading cause of death in adolescents (aged 15-24 years). Suicide among younger adolescents (aged 10-14 years) is rare but increasing. The rate of adolescent suicide in the United States tripled between 1952 and 1992. U.S. Surgeon General issued a National Strategy for Suicide Prevention on May 2001, laying out 11 goals designed to reduce and prevent this problem. Female adolescents attempt suicide nearly twice as frequently as male adolescents, although male adolescents have higher completion rates. 19% of students in grades 9-12 reported having seriously considered attempting suicide in the past year, and 14.8% reported having made a specific plan. The majority of all adolescent suicides are committed by whites, but suicide rates are significantly higher than national rates among Native Americans, and increasing rapidly among blacks. Firearms are the most commonly used method for completed suicides both among male and female adolescents. Firearms account for 62% of the increase in overall suicide rates for 15-19 years olds; one factor that may explain the prominent role of firearms in adolescent suicide is the high rate of gun ownership. 35% of U.S. households now contain a gun, and studies have shown that adolescents who commit suicide by firearms are significantly more likely to have a firearm in their home. Poisoning (including drug overdose) is a common method among female adolescents, and is thought to be the most frequent method of attempted suicide. Risk factors for suicide and suicide attempt include: presence of mental disorder; family history of psychiatric disorder; substance abuse; previous suicide attempt; certain physical disorders that cause functional impairment; history of sexual or physical abuse; easy access to lethal weapons; living in a non-traditional setting; being gay, lesbian or bisexual; stressful life events; being pregnant or parenting; being divorced; and exposure to a recent suicide or suicide attempt in a family, community or peer group, or through media coverage. All adolescents, especially pregnant or parenting adolescents, should be asked about a history of childhood sexual or physical abuse and evaluated for their risk for suicidal ideation and attempt.
Depression is associated very strongly with suicide. The defining symptoms of depression are five or more of the following (including at least 1 of the first 2) nearly everyday, all day, and for at least 2 weeks: depressed mood; diminished interest or pleasure; weight loss when not dieting or weight gain; insomnia or hypersomnia; fatigue or loss of energy; psychomotor agitation or retardation; feeling of worthlessness or excessive or inappropriate guilt; indecisiveness or diminished ability to think or concentrate; and recurrent thoughts of death, suicidal ideation, suicide attempt, or plan. Depression in adolescents, however, may not have the same clinical manifestations as in adults and may present as: somatic complaints; irritability; social withdrawal. Sexual acting-out also may be a symptom of depression and may cause the adolescent to come to the attention of the obstetrician-gynecologist. Questions should be asked in non-judgmental, direct, and non-threatening manners, such as: Have you ever thought about suicide? Are you thinking about suicide now? Do you have a plan for committing suicide? If yes, What is your plan for committing suicide? Have you ever attempted suicide? A positive response indicates the need for further questioning and an assessment of risk factors that could increase the suicide potential, such as easy access to a lethal weapon. The degree of risk at any particular encounter should, to the extent possible, be fully assessed, and any response or intervention should be based on the level of risk. Significant insight is gained into the intent of the suicidal thought by analyzing the method and location of a planned suicide.
Counseling techniques for the suicidal adolescent should emphasize that the patient's current emotional state is temporary and treatable, offering alternatives to deal with the problem. "No-suicide" contracts in which the adolescent pledges not to attempt suicide often are helpful but should not be relied on to prevent a suicide. Adolescents frequently request that their suicidal thoughts not be revealed. It is important to avoid being sworn to secrecy or making promises that cannot be kept because suicidal intent is not information that can be kept confidential. Moreover, it is imperative that, where applicable, the family of an adolescent at risk be advised immediately to make firearms in the home inaccessible and to lock up all medications kept away anywhere in the home.
Adolescent Health Research:
The risks of exposure to violence, human immunodeficiency virus (HIV), and other sexually transmitted diseases; alcohol, tobacco, and prescribed and illicit drug use; and unintended pregnancy, among others, threaten the health and well-being of adolescents in the United States and other countries. Research is needed in these and other areas to improve adolescent health care and to aid in health policy decisions. Adolescents often are prevented from participating in such research because of inadequate understanding of their legal status and the ethical considerations regarding their participation in research. In the federal regulations governing research, children are defined in 45 CFR 46 Section 102(a) as "persons who have not attained the legal age for consent to treatments or procedures involved in the research, under the applicable law of the jurisdiction in which the research will be conducted". This definition refers to laws, primarily state laws related to consent for treatment of minors, age of majority, and emancipation status. When considering the legal complexities of adolescent health research, it is important to recognize that the age of majority in almost every state is 18 years, and all states recognize the concept of emancipated minors, who generally are allowed to consent for their own health care, whether or not they are legally emancipated. A basic criterion for ethical research is the protection of the rights and welfare of people participating in research.
Under the following circumstances it is reasonable to waive parental permission when adolescents are involved in studies: a) the waiver would not adversely affect the rights and welfare of the adolescent, b) the study poses no more than a minimal risk to adolescents, c) the study could not be practically carried out without waiver, and d) requiring permission may not be reasonable to protect subjects. Parental permission is not a requirement for research involving the provision of health care for which adolescents do not legally need parental consent. Researcher conducting and Institutional Review Boards (IRBs) reviewing research involving adolescents should be knowledgeable of the federal regulation and the ethical principles that underlie these regulations. They should understand when parental permission is required and when it may be waived. Personal beliefs and attitudes should not enter into this decision.
Editor's Note:
Institutional procedures that safeguard the rights of the adolescent patients, including confidentiality during initial and subsequent visits and in billing, should be established. Billing mechanisms for services and procedures for insurance and other third-party reimbursement should ensure adolescent confidentiality. When these mechanisms and procedures compromise a patient's request for confidentiality, policies should be implemented allowing payment alternatives such as referral fees, sliding scales, and timed installed payments and patient referral to a practice or agency where subsidized care is offered or both. Efforts to encourage young people to delay becoming sexually active are components of almost all sexuality education programs. Communities planning appropriate sexuality education for adolescents should consider parental involvement in their child (ren)'s sexuality education and all sexuality education programs should provide scientifically accurate information about sexuality, STDs, contraception, and preventive health care.
Overweight status in the adolescent female population has been associated with lower educational achievement and income, even after controlling for intelligence and socioeconomic status at baseline. We also recommend that all adolescents be screened annually for overweight by determining weight and stature, calculating a body mass index for age percentile, and asking about body image and eating patterns. Healthcare providers should promote healthy eating and physical activity to adolescent patients and their parents during routine preventive health care visits. Sound nutritional recommendations and regular physical activity are essential for overall good health because they convey myriad benefits for growth, brain and cognitive development, self-esteem, immunity, and disease prevention. Additional research is needed to determine the most appropriate approach the successful prevention and treatment of overweight adolescents. The idea of "health at any size" encourages patients to focus on their overall health improvement, rather than only their weight status.
Physicians have an important role in addressing the problem of adolescent suicide. The increasing rate of adolescent suicide mandates an increasing awareness of depressive disorders, anxiety disorders, and chemical dependence in this population. Physicians should be prepared to assess suicide risk and when necessary, provide immediate counseling or referral to mental health providers. Each patient encounter may be the only opportunity of intervention and may in fact be life saving.
Resources & Suggested Reading:
- World Health Organization
Child and Adolescent Health and Development - American Academy of Pediatrics
Section of Adolescent Health - Society for Adolescent Medicine
Advancing health and wellbeing of adolescents - Center for Adolescent Health and the Law
Policy Compendium on Confidential Health Services for Adolescent - Teenwire (by Planned Parenthood Federation of America)
List of teen events of Planned Parenthood
Published: 23 September 2009
Dedicated to Women's and Children's Well-being and Health Care Worldwide
www.womenshealthsection.com