Текущий Управление Рак яичниковWHEC практики Бюллетень и клинических управления Руководство для медицинских работников. Образования гранта, предоставленного здоровья женщин-образовательный центр (WHEC). Epithelial ovarian cancer is the second most common gynecologic malignancy, but is the leading cause of death from gynecologic cancer in the United States. These practice guidelines are a statement of consensus of the authors regarding their views on currently accepted approached to treatment. In 2013, an estimated 22,200 new diagnoses of and 14,000 deaths from ovarian cancer will occur in the United States (1). This discussion addresses the most common type of ovarian cancer. The four main histologic subtypes of epithelial ovarian cancer are serous, endometrioid, mucinous, and clear cell; however, most patients (~70%) have serous histology (2). Although some histologic subtypes respond differently, recommended primary treatment for these histologic subtypes does not currently differ; all are treated using the recommendations for epithelial cancer (3). Less common cancers, such as fallopian tube cancer and primary peritoneal cancer are managed in a similar manner to epithelial ovarian cancer. Less common ovarian histopathologies are also described, including malignant germ cell neoplasms, carcino-sarcomas (malignant mixed Müllerian tumors of the ovary [MMMT]), and sex cord-stromal tumors. Another less common ovarian neoplasia is borderline epithelial ovarian tumor, which is less sensitive to chemotherapy than epithelial ovarian cancer, and in general, is managed surgically like malignant ovarian cancer except in specific circumstances. The purpose of this document is to integrate into professional practice the updates for management of ovarian cancer. It also describes the rationale behind the decision-making process for developing these guidelines. In this discussion four updates are selected based on recent important updates in the guidelines and on debate among the experts about recent clinical trials. The topics include: 1) intraperitoneal (IP) chemotherapy, 2) CA-125 monitoring for ovarian cancer recurrence, 3) surveillance recommendations for less common ovarian histopathologies, and 4) recent changes in therapy for recurrent epithelial ovarian cancer. During primary surgery for advanced stage epithelial ovarian cancer all attempts should be made to achieve complete cytoreduction. When this is not achievable the surgical goal should be optimal (<1cm) residual disease. Due to high risk of bias in the current evidence, randomized controlled trials should be performed to determine whether it is the surgical intervention or patient-related and disease-related factors that are associated with the improved survival in these groups of women. The findings of current reviews is that women with residual disease <1cm will do better than women with residual disease >1cm should prompt the surgical community to retain this category and consider re-defining it as “near optimal” cytoreduction, reserving the term “suboptimal” cytoreduction to cases where the residual disease is >1cm (optimal/near optimal/suboptimal instead of completer/optimal/suboptimal). Optimal cytoreduction (defined as microscopic) is associated with improved survival. The ability to achieve optimal cytoreduction is likely a factor of tumor biology and surgeon aggressiveness. There is no reliable way to predict pre-operatively the ability to achieve optimal cytoreduction. Secondary cytoreduction, in the appropriate patient population, may be associated with improved survival. Pathologic Staging and Primary Chemotherapy / Primary Adjuvant TherapyOvarian cancer has been separated into histological categories. Specific molecular features begin to define these categories: 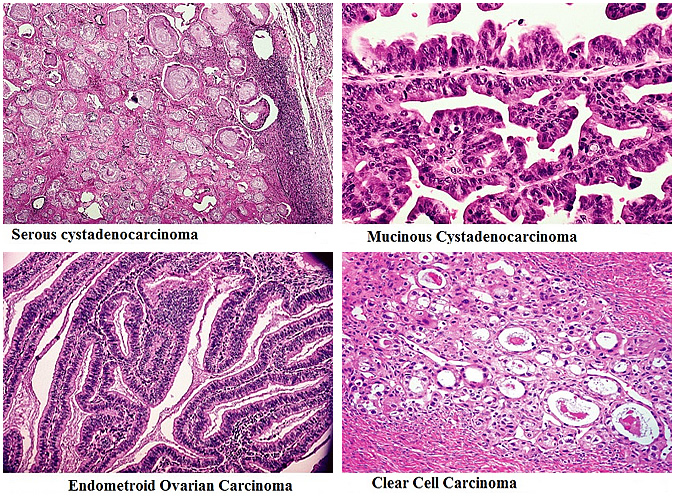
Patients with early stage disease need to have comprehensive surgical staging to assess risks and to direct adjuvant chemotherapy. In addition, for advanced ovarian cancer, primary surgical cytoreduction plays an important role. The goal of cytoreduction surgery is to achieve optimal tumor reduction, ideally with individual aggregates of residual disease less than 1 cm. All women undergoing surgery for ovarian cancer should be counseled about the clinical benefit associated with combined intravenous (IV) and intraperitoneal (IP) chemotherapy administration prior to surgery. Surgical cytoreduction (debulking) is recommended as initial treatment for many women with ovarian cancer, even those with metastatic disease (4),(5). After surgical debulking, adjuvant systemic therapy (e.g. taxane/platinum) is recommended for many patients (6). Several different systemic regimens are recommended (7). Primary adjuvant therapy regimens include intravenous (IV) with (or without) intraperitoneal (IP) options. All of the regimens may be used for epithelial ovarian, primary peritoneal, and fallopian tube cancers. Stage IA or IB
Stage IC
Stage II, Stage III, Stage IV
Monitoring and Follow-up
Intraperitoneal (IP) ChemotherapyIP as a therapeutic strategy for patients with ovarian cancer was based on pharmacologic modeling studies performed in the late 1970s (8). The rationale was based on the findings of high intraperitoneal concentration of drugs and longer half-life of the drug in the peritoneal cavity, which resulted in a prolonged exposure of the chemotherapy agents. One of the concerns of the use of IP chemotherapy has been uniform distribution of the drug, which may not occur because of adhesions that result from surgery. IP chemotherapy is recommended (category 1) for selected stage III patients with optimally debulked (<1 residual) disease (i.e. low-volume residual disease) based on randomized controlled trials (9). Patients with optimally debulked stage II disease may also receive IP chemotherapy, although no randomized evidence has been published; therefore, this is a category 2A recommendation (10). However, IP chemotherapy is not recommended for patients with stage I and IV disease in the recent guidelines. In women with stage II cancer who had residual disease measuring less than 1 cm after debulking, survival was increased by 16 months after IP therapy using cisplatin/paclitaxel when compared with standard IV therapy. Recent long-term follow-up data have confirmed this extraordinary survival advantage (11). Overall survival was 110 months in patients with stage III ovarian cancer and no residual disease was found in those who received IP regimen (11). Although whether to use IP chemotherapy (vs. IV chemotherapy alone) may be difficult, the excellent survival rates for IP chemotherapy makes this a valid option for selected patients (12). Women with primary peritoneal cancer, fallopian tube cancer, or MMMT can also be considered for IP chemotherapy, although MMMT has not been included in IP chemotherapy trials (13). However, MMMT/carcinosarcoma is basically papillary serous carcinoma (i.e. a poorly differentiated carcinoma); therefore, IP may be used for MMMT. Potential toxicities associated with the IP paclitaxel/cisplatin regimen include leukopenia, infection, fatigue, renal toxicity, abdominal discomfort, neurotoxicity, and catheter complications (14). Patients with poor performance status, comorbidities, or advanced age may not tolerate the IP regimen. Patients with stage IV disease have generally not been included in randomized trials of IP therapy; thus, its benefits have not been demonstrated in this group. Strategies to decrease toxicity and improve compliance with the IP chemotherapy regimen include using carefully selected patients, modifying dose and/or schedule, decreasing catheter complications, and using expert nursing care. The recommended IP chemotherapy regimen is paclitaxel 135 mg/m2 continuous intravenous infusion over 3 or 24 hours on day 1; cisplatin 75 to 100 mg/m2 IP on day 2 after IV paclitaxel; and paclitaxel 60 mg/m2 IP on day 8; repeated every 3 weeks for 6 cycles (category 1) (15). Note that this IP chemotherapy regimen includes IV paclitaxel, so that systemic disease can also be treated. The published randomized trial for this IP chemotherapy regimen used IV continuous infusion of paclitaxel over 24 hours (15). Revised regimen in 2013, includes a 3-hour infusion of paclitaxel, because it has been reported to be more convenient, easier to tolerate, and less toxic that a 24-hour infusion (16). However, a randomized trial comparing a 3-hour versus a 24-hour infusion of paclitaxel has not been performed to determine whether they are equivalent. Using a lower IP cisplatin dose of 75 mg/m2 or splitting the dose may also help to decrease toxicity (16). Previously, capping doses at a maximum body surface area of 2.0 m2 was recommended to reduce toxicity; however, this restriction was deleted in the 2013 update. If obese women receive doses based on their actual body weight, data suggest that they do not experience more toxicity; therefore, dose capping does not seem to be necessary and may result in suboptimal treatment. Women should receive IV therapy if they are unable to complete IP chemotherapy necessary to maintain a survival advantage is unclear, although recent data suggest that survival correlates with the number of IP cycles received (17). After 5 years, more women who received 5 or 6 cycles of IP chemotherapy were alive (59%) than those who only received 3 or 4 cycles (33%) or even 1 to 2 cycles (18%) (18). Primary Chemotherapy/Primary Adjuvant Therapy Regimens for Stage II-IV
Monitoring/Follow upStage I, II, III and IV Complete Response
PET: Positron Emission Tomography; CT: Computed Tomography; MRI: Magnetic Resonance Imaging Recurrent Disease
CA-125 Monitoring for Ovarian Cancer RecurrenceRecurrence is mostly detected by rises in CA-125 levels. Patients who have been treated for ovarian cancer and have experienced a complete response are carefully followed (monitored) to determine whether the disease has recurred. Monitoring includes measuring blood CA-125 levels if they were initially increased, physical and pelvic examinations, and other tests if indicated, such as imaging (19). For asymptomatic patients with only biochemical evidence of relapse (i.e. with increased CA-125 levels but without radiographic and/or clinical evidence of relapse), treatment options include delaying treatment until clinical evidence of relapse (category 2A) or providing immediate treatment (category 2B). This study (20) and expert panel recommend (category 2A) that treatment should be delayed until clinical evidence of relapse (e.g. ascites, abdominal/pelvic/back pain/weight loss, bloating, and obstruction) based on a recent European trial. A recent multi-institutional European trial assessed the use of CA-125 monitoring for ovarian cancer recurrence after primary therapy (20). Data suggest that treating recurrences early (based on detectable CA-125 levels in otherwise asymptomatic patients) is not associated with an increase in survival, and is associated with an increase in survival, and is associated with decrease in quality of life (21). We suggest that the patients the pros and cons of CA-125 monitoring with their physicians. However, patients often prefer to have CA-125 monitoring. Several articles discuss CA-125 monitoring in greater detail (22). Acceptable Recurrence Therapies (1 of 2) †
†Patients who progress on two consecutive therapy regimens without evidence of clinical benefits have diminished likelihood of benefiting from additional therapy. Decisions to offer clinical trials, supportive care, or additional therapy should be made on a highly individual basis. Therapy for Recurrent DiseaseThe definition of “recurrence” is not standard. Recurrence is divided into three categories:
Although most patients with ovarian cancer experience a response to initial treatment, 75% to 80% will experience a relapse of their disease (23). Patients with ovarian cancer will often receive multiple types of recurrence therapy, because their disease frequently responds to sequential therapies. Recurrence therapy for patients with epithelial ovarian cancer, fallopian tube cancer, and primary peritoneal cancer a new preferred regimen has been suggested – carboplatin/gemcitabine/bevacizumab (category 2B), based on the recent OCEANS trial (24). This phase III randomized trial assessed carboplatin/gemcitabine with and without bevacizumab in patients with platinum-sensitive recurrent ovarian cancer who had not previously received bevacizumab. In patients receiving the chemotherapy/bevacizumab arm, progression-free survival increased when compared with chemotherapy alone, 12.4 vs. 8.4 months (25). However, overall survival was not increased in the chemotherapy/bevacizumab arms. Combination therapy with bevacizumab is a category 2B recommendation, because there is less consensus that this intervention would be routinely used by the panel members. Many of the experts feel that other combination regimens may be more beneficial and effective than those with bevacizumab. In addition, the carboplatin/gemcitabine/bevacizumab regimen is only recommended in patients who have not previously received bevacizumab. Based on 2 phase II trials, bevacizumab alone is potentially active in patients who have recurrent disease (especially those with ascites), which is reflected in the category 2A recommendation for single-agent bevacizumab (26). Surveillance Recommendations for less common Ovarian HistopathologiesMalignant germ cell tumors and sex cord-stromal tumors are rare. The following are updates in recommendations based on the data from the Society for Gynecologic Oncology (27). The recommendations are different for the two types of tumors, because sex cord-stromal tumors can recur many years after initial diagnosis and treatment. Surveillance for Germ Cell and Sex Cord-Stromal Tumors
*Chest X-ray, CT, MRI WHEC Categories of Evidence and ConsensusCategory 1: Based upon high-level evidence, there is uniform WHEC consensus that the intervention is appropriate. All recommendations are Category 2A unless otherwise noted. Clinical trials: WHEC believes that the best management for any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged. SummaryThese update topics include: IP chemotherapy; CA-125 monitoring for ovarian cancer recurrence; surveillance recommendations for less common ovarian histopathologies, and recent changes in therapy for recurrent disease (mainly epithelial ovarian cancer). After initial surgery, IP is recommended (category 1) for selected stage III patients with low-volume residual disease. For the 2013 update, the dosing for the IP chemotherapy regimen was revised to include a 3-hour infusion of paclitaxel, because it has been reported to be more convenient, easier to tolerate and less toxic. However, a 3-hour infusion of paclitaxel has not been proven to be equivalent to a 24-hour infusion in a randomized controlled trial. Previously, capping doses at a maximum body surface area of 2.0 m2 was recommended to reduce toxicity; however, for the 2013 update, this restriction was deleted. If obese women receive doses based on their actual body weight, data suggest that they do not have increased toxicity; therefore, dose capping does not seem to be necessary and may result in suboptimal treatment. Patients who have been treated for ovarian cancer and have had a complete response are carefully monitored to determine whether the disease has recurred. The treatment for ovarian cancer should be delayed until radiographic and/or clinical evidence of relapse (e.g. ascites, abdominal/pelvic/back-pain, weight loss, bloating, and obstruction). A recent trial suggests that treating recurrences early (based only on detectable CA-125 levels in otherwise asymptomatic patients) is not associated with an increase in survival but is associated with a decrease in quality of life. Therefore, early immediate treatment is only a category 2B recommendation in these new guidelines. Recurrence treatment ideally should be based on platinum sensitivity along with histology and any genomic information. For platinum sensitive cancer, a platinum doublet (or single agent platinum) should be considered. Platinum allergies occur in up to 20% of patients; desensitization protocols are successful. For platinum resistant cancer, pegylated liposomal doxorubicin, gemcitabine, bevacizumab, weekly paclitaxel or another single agent cytotoxic are possible next therapies. Surgery and radiation therapy should be considered for patients who have isolated and near solitary sites of cancer. Consideration should be made for early clinical trial for these patients. References
|